Lumbar Discectomy
 Lumbar discectomy is a surgical procedure used to treat nerve compression caused by a herniated disc in the lower back.
Lumbar discectomy is a surgical procedure used to treat nerve compression caused by a herniated disc in the lower back.
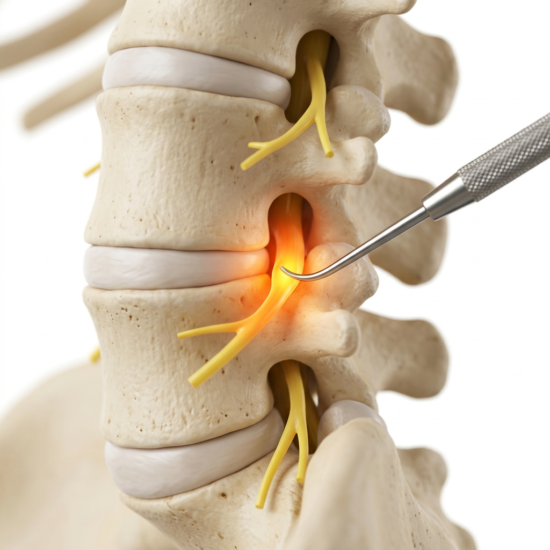
When a portion of the disc presses on a nerve root, it can cause radicular pain—most commonly felt in the leg (sciatica), but often also in the buttock. Many patients describe this as “back pain,” when in reality it is nerve-related pain located in the buttock and radiating in a characteristic pattern. Some patients can also have localized back pain, along the same side as their pinched nerves. While generalized back pain suggests more structural and mechanical sources of pain.
The goal of surgery is to relieve pressure on the nerve and allow it to recover.
When Is It Indicated?
Lumbar discectomy is most appropriate when the primary issue is nerve compression, and the overall integrity of the disc remains preserved.
Not all disc herniations are the same. Focal disc extrusions that compress a single nerve root behave very differently from broad-based disc bulges that narrow the spinal canal and affect multiple nerves. In the latter case, the disc may have lost its structural integrity, and a simple discectomy may not be sufficient.
Lumbar discectomy is best suited for cases involving:
- Predominant radicular pain (leg or buttock pain) rather than true mechanical low back pain
- Minimal or no discogenic pain
- Focal nerve compression corresponding to imaging findings
- Failure of appropriate non-operative treatment
When symptoms are primarily due to isolated nerve irritation—and not structural failure of the disc—targeted decompression can be highly effective.
What Does the Procedure Involve?
 The procedure involves removing the portion of the disc that is compressing the nerve.
The procedure involves removing the portion of the disc that is compressing the nerve.
Whenever possible, only the offending fragment is removed (sequestrectomy), preserving the remainder of the disc. In some cases, however, the annulus (outer layer of the disc) has a larger defect, and the nucleus (inner disc material) may be exposed. In these situations, the disc space may need to be carefully explored to remove additional loose fragments and reduce the risk of ongoing or recurrent compression.
The extent of disc removal is individualized based on the structure and integrity of the disc.
Our Approach
 Our goal is to relieve nerve compression while preserving as much of the normal disc and surrounding structures as possible.
Our goal is to relieve nerve compression while preserving as much of the normal disc and surrounding structures as possible.
When appropriate, we use minimally invasive or endoscopic techniques to target the pathology with minimal disruption to normal anatomy. The decision between limited fragment removal and more extensive decompression is based on intraoperative findings and the condition of the disc.
Limitations and Considerations
Lumbar discectomy is most effective for radicular symptoms caused by nerve compression.
It is less effective for isolated mechanical low back pain, where the disc itself may be a source of symptoms. In these cases, other treatment strategies may be more appropriate.
There is a risk of recurrence, as the remaining disc can herniate again over time. This risk is influenced by several factors, including:
- The size of the annular defect
- The height and overall health of the disc
- The inherent structural integrity of the disc
Postoperative rehabilitation and correction of contributing biomechanical factors are important in reducing this risk. Improving spine hygiene, posture, and movement patterns—and reinforcing these through patient-specific exercises—can help address some of the underlying stresses that may have contributed to the herniation in the first place. This also plays an important role in preserving the health of adjacent spinal levels over time.
At the same time, rehabilitation cannot completely prevent recurrence. Once a disc has herniated, it has already demonstrated a degree of structural vulnerability, and in some patients it may re-herniate despite excellent recovery and careful correction of mechanical factors. The goal of rehabilitation is therefore not to guarantee prevention, but to reduce recurrence risk as much as possible and support long-term spine health.